Literature Sharing: Tumor Immune Evasion Mechanisms and Counterstrategies
This article systematically analyzes the review "Immune evasion in cell-based immunotherapy: unraveling challenges and novel strategies" published by Li et al. in the Journal of Biomedical Science. The literature focuses on the core challenge of tumor immune evasion in Cell-based Immunotherapies (CBIs), systematically integrating recent basic research and clinical data related to tumor immune evasion and CBIs, forming a complete research system of "evasion mechanisms - counterstrategies - biomarkers", which provides important support for the optimization of CBIs.
1. Overview of Research Background
Cell-based immunotherapy represents a revolutionary breakthrough in cancer treatment. Its core principle is to modify immune cells ex vivo, activate and reinfuse them, enabling the body's own immune system to precisely kill tumor cells. This represents a new direction in personalized precision cancer treatment. Cell-based immunotherapies, represented by CAR-T and CAR-NK, use genetic engineering to equip immune cells with the ability to specifically recognize tumor antigens and enhance their cytotoxic effects. They have demonstrated unprecedented efficacy in previously intractable malignancies, significantly breaking through the limitations of traditional chemotherapy, radiotherapy, and targeted therapy.
Despite the landmark successes of CBIs in hematologic malignancies, several bottlenecks remain in clinical application: off-target effects, limited efficacy in solid tumors, tumor immunosuppressive microenvironment, and unstable cell manufacturing processes have severely restricted their widespread use. Among these, tumor immune evasion is the most critical factor leading to CBI treatment failure and disease recurrence. Tumors can evade attack by engineered immune cells through multiple strategies: (1) downregulating or losing target antigens, reducing the probability of being recognized by immune cells; (2) highly expressing immune checkpoint molecules such as PD-L1, directly inhibiting immune cell activation; (3) constructing a highly immunosuppressive tumor microenvironment (TME), recruiting inhibitory immune cells, secreting immunosuppressive factors, and systematically weakening immune responses; (4) inducing immune cell exhaustion and functional abnormalities, making it difficult for CBIs to exert sustained anti-tumor effects.
Therefore, systematically dissecting the immune evasion mechanisms of tumors against CBIs, clarifying key links such as TME regulation, antigen expression loss, and inhibitory signal activation, and exploring optimized strategies such as combination therapy, checkpoint blockade, and gene editing to reverse immune evasion, are of crucial scientific significance and clinical value for improving CBI efficacy, prolonging patient survival, and promoting clinical translation of cell-based immunotherapy.
2. Main Mechanisms of Tumor Immune Evasion
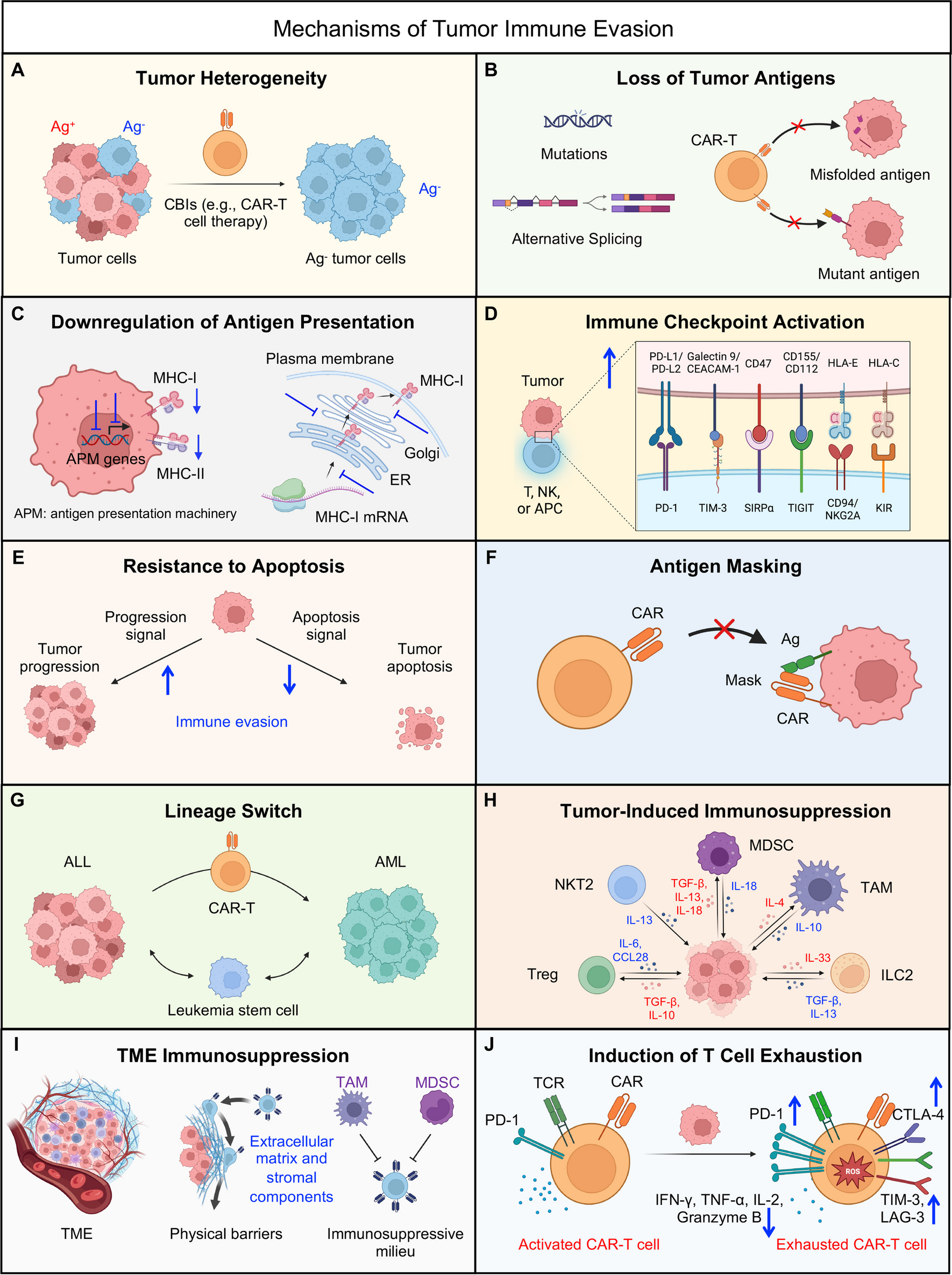
In the literature, the authors systematically categorized tumor immune evasion mechanisms into ten major types, covering three core levels: changes in tumor cell characteristics, TME regulation, and immune cell dysfunction. These mechanisms cooperate and interact with each other, forming a complex immune evasion network.
Evasion Mechanisms Related to Changes in Tumor Cell Characteristics
1. Tumor Heterogeneity
Within the same tumor, there are significant differences in cell phenotypes and genes. Some cancer cells inherently lack therapeutic targets (e.g., CD19-negative subpopulations). After CAR-T treatment, these cells rapidly proliferate, leading to recurrence and making single-target therapy unable to completely eliminate tumors.
2. Tumor Antigen Loss
This is the most common evasion mechanism. Cancer cells use gene mutations and abnormal splicing to make target antigens such as CD19 and BCMA absent, functionally abnormal, or unable to be expressed on the cell surface, directly evading immune cell recognition.
3. Downregulation of Antigen Presentation
Cancer cells reduce MHC molecule expression, interfere with antigen processing and transport, and decrease co-stimulatory molecules, preventing antigens from being properly presented to immune cells. Even if targets exist, they are difficult to be recognized and activated.
4. Enhanced Apoptosis Resistance
Cancer cells highly express anti-apoptotic proteins such as Bcl-2 and Bcl-xL, inhibiting immune cell-induced apoptosis and enabling survival and proliferation even when attacked.
5. Antigen Masking
The surface of cancer cells is covered by structures such as CARs and sialomucins, masking target antigens and preventing immune cells from binding and recognizing them, leading to treatment failure.
6. Lineage Switch
Commonly seen in MLL-rearranged leukemia, cancer cells undergo phenotypic transformation under immune pressure, losing original targets and converting to other cell types, rendering CAR-T completely ineffective.
Evasion Mechanisms Related to Tumor Microenvironment (TME) Regulation
1. Infiltration of Immunosuppressive Cells
Tumors recruit inhibitory cells such as TAMs, MDSCs, and Tregs, which secrete inhibitory factors and express PD-L1, directly suppressing the activation and killing functions of immune cells.
2. Secretion of Immunosuppressive Molecules
Tumors release large amounts of substances such as TGF-β, IL-10, and adenosine, comprehensively inhibiting immune cell function while promoting tumor invasion, forming an immunosuppressive environment.
3. Extracellular Matrix (ECM) Barrier
Tumors over-secrete collagen and proteoglycans, forming a dense physical barrier that blocks immune cells from entering the tumor interior to function.
4. Abnormal Angiogenesis
Tumor blood vessels have disorganized structures and poor permeability, hindering immune cell infiltration. At the same time, hypoxia is induced, further upregulating inhibitory molecules such as PD-L1, forming a vicious cycle.
Evasion Mechanisms Related to Immune Cell Dysfunction
1. Immune Checkpoint Activation
Tumors highly express checkpoint molecules such as PD-L1, CTLA-4, and TIM-3. When bound to immune cells, they transmit inhibitory signals, directly shutting down the killing ability of immune cells.
2. T Cell Exhaustion
Chronic tumor stimulation combined with inhibitory microenvironment leads to decreased T cell function, reduced cytokine secretion, and sustained high expression of inhibitory receptors, resulting in loss of anti-tumor ability. Some function can be restored through checkpoint blockade.
3. Multiple Strategies to Counter Tumor Immune Evasion
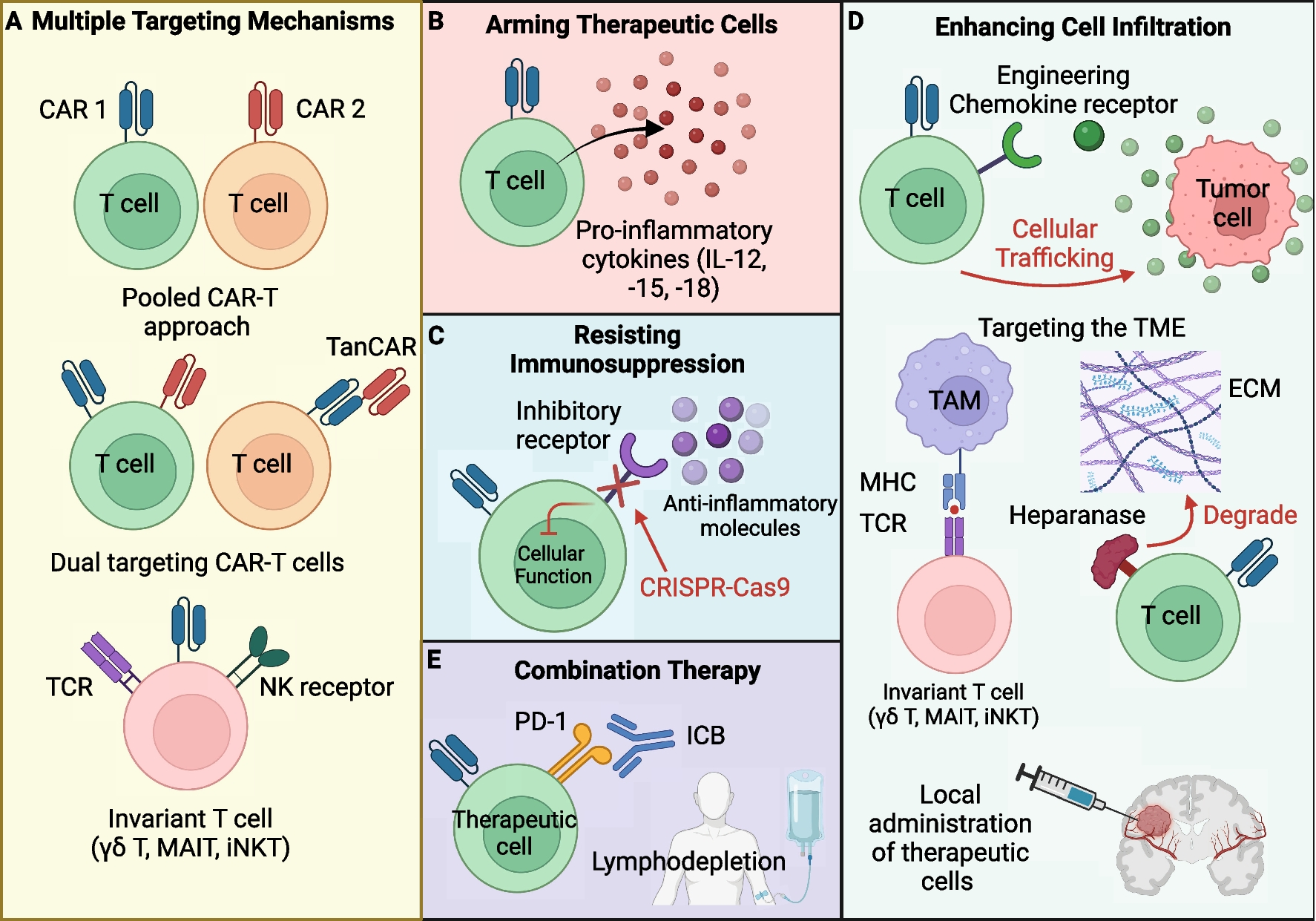
In response to the core mechanisms of tumor immune evasion described above, the article proposes five categories of targeted engineering strategies, focusing on enhancing the tumor recognition ability, survival ability, TME infiltration ability, and functional maintenance ability of CBIs. Through multi-dimensional, systematic modifications, these strategies aim to break the tumor immune evasion network and improve the therapeutic effect of CBIs.
Multi-Target Engineering: Overcoming Antigen Escape and Tumor Heterogeneity
The core idea is to recognize multiple tumor antigens simultaneously, reducing the probability of evasion.
1. Multi-target CAR Engineering: Using mixed CAR-T, dual-target CAR, and tandem CAR (TanCAR) technologies to enable immune cells to recognize two targets simultaneously. Clinical remission rates can reach 70%-86%, significantly reducing recurrence caused by antigen loss.
2. Using Unconventional Immune Cells: Cells such as NK, iNKT, and γδT can recognize tumors through their own receptors without relying on MHC antigen presentation, effectively countering antigen downregulation or loss, making them suitable for CAR engineering.
Enhancing Therapeutic Cell Persistence: Countering T Cell Exhaustion and Immunosuppression
Modify cells to extend their survival and activity in vivo.
1. Cytokine Armoring: Engineering CAR-T to secrete IL-15, IL-18, etc., enhancing proliferation, reducing apoptosis, and decreasing PD-1 expression. Currently, inducible secretion is commonly used to avoid cytokine storm toxicity.
2. Memory Phenotype Induction: Inducing CAR-T into stem cell-like/central memory phenotypes (high expression of CD27, CD45RO) to enhance persistence and long-term anti-tumor ability.
Resisting TME Immunosuppression: Breaking the Inhibitory Signal Network
Directly make therapeutic cells "immune" to inhibitory signals and eliminate inhibitory cells.
1. Blocking Inhibitory Pathways: Using CRISPR to knockout TGF-β receptors, adenosine A2A receptors, or expressing dominant negative receptors, making CAR-T unaffected by inhibitory molecules such as TGF-β and adenosine.
2. Eliminating Inhibitory Cells: Engineering immune cells to target and eliminate immunosuppressive cells such as TAMs and MDSCs, reshaping the tumor microenvironment.
Enhancing Infiltration Ability: Breaking Through Tumor Physical Barriers
Solve the problem of immune cells unable to enter the tumor interior.
1. Chemokine Receptor Engineering: Overexpressing receptors such as CXCR2, CCR6, and CCR2b to guide CAR-T to migrate and accumulate precisely towards tumors.
2. Matrix Degradation: Engineering CAR-T to express heparanase (HPSE) to degrade extracellular matrix and open channels into tumors.
3. Local Delivery: Directly injecting CAR-T into tumor regions to increase local concentration and improve efficacy.
Combination Therapy: Synergistic Enhancement, Comprehensive Breakthrough
Single strategies are insufficient; combinations work better.
1. + Immune Checkpoint Inhibitors: Release PD-1/PD-L1 inhibition to restore T cell function.
2. + Chemoradiotherapy: Radiation enhances immunogenicity and destroys barriers; chemotherapy eliminates inhibitory cells and facilitates CAR-T expansion.
3. + mRNA Vaccine (CARVac): Activates and expands CAR-T. Low doses can control tumors, with objective response rates of up to 33% in solid tumors.
4. Biomarkers Related to Cell-Based Immunotherapy
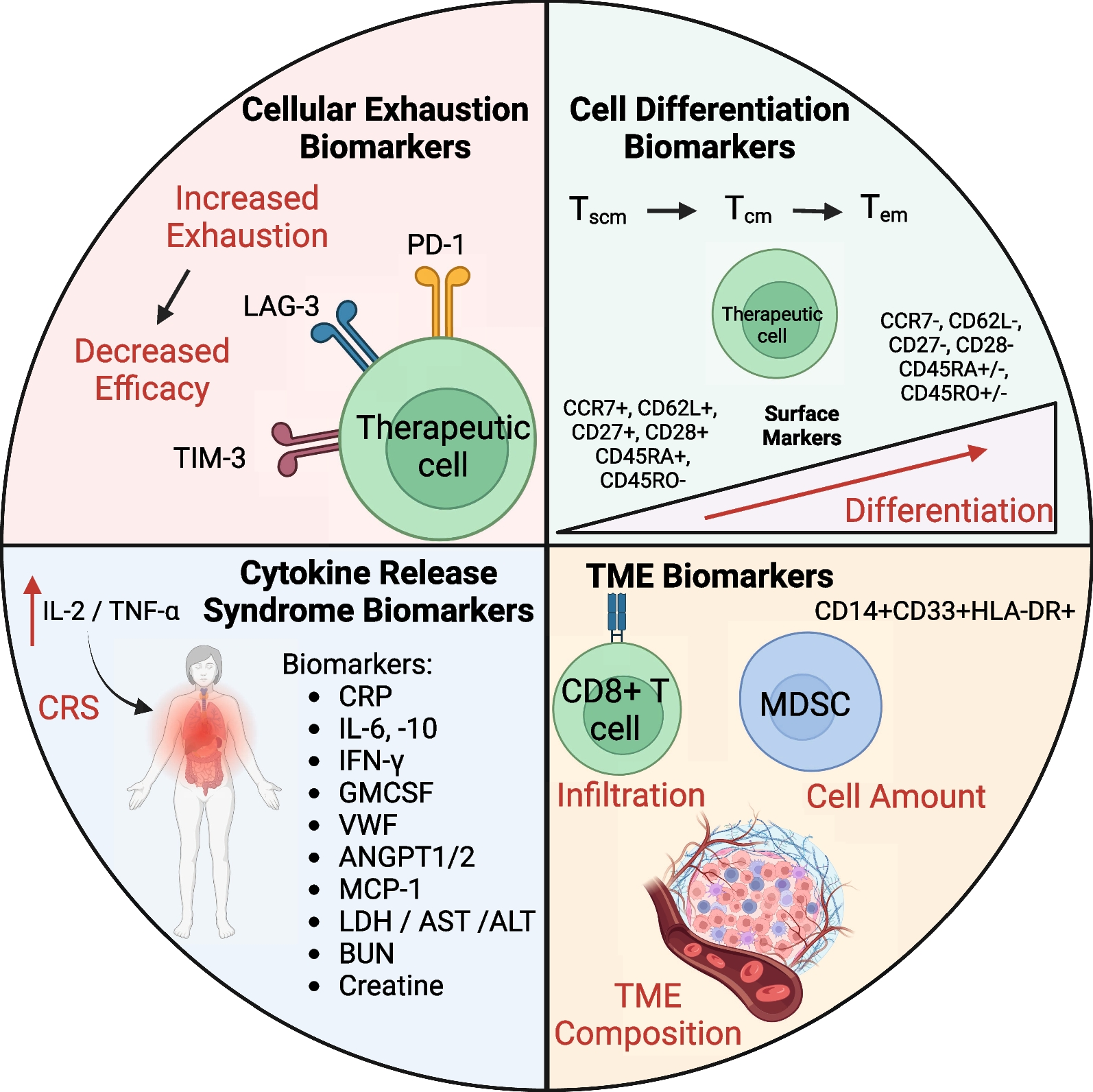
Combining tumor immune evasion mechanisms with CBI treatment characteristics, the literature systematically summarizes four categories of core biomarkers. These biomarkers can not only predict CBI treatment response, monitor adverse reactions during treatment, but also evaluate TME immune status, providing important references for formulating personalized clinical treatment plans. They are an important part of the "evasion mechanisms - counterstrategies - biomarkers" research system.
Immune Cell Exhaustion Biomarkers
Used to determine whether immune cells are "exhausted" and predict treatment efficacy.
● Core: High expression of PD-1, LAG-3, TIM-3 indicates decreased T cell function, weakened killing ability, and poor treatment outcome.
● Auxiliary: Decreased IL-2, IFN-γ, and increased IL-10 indicate aggravated immunosuppression.
● Significance: Can predict efficacy in advance and guide whether to combine with immune checkpoint inhibitors.
Immune Cell Differentiation Biomarkers
Used to assess CAR-T survival and long-term efficacy.
● Memory T cells (Tscm, Tcm, high expression of CD27, CD62L, CD45RO): Higher proportion correlates with longer CAR-T survival and lower recurrence rate.
● CD127 high expression indicates strong self-renewal ability and better resistance to tumor microenvironment inhibition.
Cytokine Release Syndrome (CRS) Biomarkers
Used to monitor the most common serious side effect of CAR-T.
● Key: IL-6 is the core indicator; higher levels indicate more severe CRS.
● Auxiliary: Increased IL-10, CRP, VWF indicate inflammation and endothelial damage, enabling early warning of severe reactions and timely intervention.
Tumor Microenvironment (TME) Biomarkers
Assess immunosuppressive strength and guide treatment plans.
● Immunosuppressive cells: Higher proportions of MDSCs, Tregs, TAMs correlate with poorer treatment efficacy.
● Inhibitory molecules: High expression of TGF-β, IL-10, PD-L1 indicates a harsh microenvironment, requiring enhanced "anti-inhibition" strategies.
● Matrix indicators: High collagen and fibronectin indicate thick barriers, requiring enhanced immune cell infiltration ability.
5. Conclusion
This review article makes significant contributions by systematically summarizing the main mechanisms of tumor immune evasion in cell-based immunotherapy, proposing multiple engineering counterstrategies, and categorizing four core cell-based immunotherapy-related biomarkers. Through clear review diagrams, it intuitively presents the complete research system of "evasion mechanisms - counterstrategies - biomarkers", with important research value and academic contributions. In terms of research value, this literature for the first time systematically integrates ten categories of tumor immune evasion mechanisms, clarifies the molecular basis and interactions of various mechanisms, filling the gaps in existing research where mechanism classification is not systematic and the correspondence between strategies and mechanisms is weak. The proposed strategies such as multi-target engineering, cytokine armoring, and TME reshaping have strong clinical translation potential, providing clear directions for the development of next-generation CBIs. The summarized biomarker system provides important references for clinical personalized treatment and efficacy monitoring, promoting the transformation of CBIs from "universal" to "personalized".
References
Li YR, Halladay T, Yang L. Immune evasion in cell-based immunotherapy: unraveling challenges and novel strategies. J Biomed Sci. 2024 Jan 12;31(1):5. doi: 10.1186/s12929-024-00998-8. PMID: 38217016; PMCID: PMC10785504.