Literature Sharing: SITC Best Practices for Multiplex Immunohistochemistry and Immunofluorescence Staining and Validation
The article "The Society for Immunotherapy in Cancer statement on best practices for multiplex immunohistochemistry (IHC) and immunofluorescence (IF) staining and validation" was led by the Pathology Working Group of the Society for Immunotherapy of Cancer (SITC), co-authored by pathologists from academic institutions, laboratory directors, and experts from pharmaceutical and diagnostic companies, and published in the "Journal for ImmunoTherapy of Cancer", focusing on optimal operation specifications for multiplex immunohistochemistry (mIHC) and multiplex immunofluorescence (mIF) staining and validation. The immune characteristics of the tumor microenvironment (TME) are closely related to cancer prognosis and immunotherapy response. mIHC/mIF technology can quantify immune cell subsets, functional states, and spatial distribution, but its application has problems such as large platform differences and non-standardized operations. To this end, SITC convened experts from multiple fields to sort out the principles, processes, advantages and disadvantages of various mIHC/mIF technologies, formulate consensus recommendations for antibody selection, experimental optimization, validation and other links, and point out that this technology is expected to enter routine clinical applications, providing an important reference for its standardized development and biomarker research.
I. Research Background and Purpose
The tumor microenvironment (TME) is a collection of complex interactions between host components and tumor cells, including various immune cells, cells with specific immune active protein expression patterns, and stromal cells, each of which constitutes a unique microenvironment niche. Studies have shown that tumor or immune cell PD-L1 expression, pretreatment CD8+T cell infiltration density and other TME characteristics are related to immune checkpoint inhibitor treatment response. Studies of samples during treatment also provide important basis for clarifying the remodeling effect of immunotherapy on TME, drug mechanisms, and early markers of efficacy. Based on this, characterizing more TME features to explore reliable biomarkers and promote precision medicine has become a research hotspot.
Currently, the most clinically valuable biomarkers come from tumor-associated cell analysis, while peripheral blood immune cell characterization has low correlation with TME cell composition and limited value in screening patients who benefit from immunotherapy. Tumor sample research faces challenges such as scarce tissue resources, differences in pre-processing of paraffin embedding, spatial heterogeneity of marker expression, and difficulty in in situ detection of complex or rare cell phenotypes. Flow cytometry is suitable for cell phenotype analysis, but relies on fresh tissue, has low cell yield and loses spatial information, limiting its routine application.
The multi-omics approach adopted by the TCGA project provides a large amount of data, facilitating tumor classification and research on the prognostic significance of immune infiltration, but samples include non-tumor tissue. Although bioinformatics analysis can achieve virtual single-cell analysis, it still loses spatial information, and single-cell RNA-seq also lacks spatial context. In contrast, immunohistochemistry (IHC) can distinguish different cells expressing the same protein, characterize the density and spatial distribution of specific cells in the TME, and semi-quantitatively assess marker intensity. Immunofluorescence (IF) can characterize expression with a wide dynamic range at the single-cell level. The core of IHC and IF detection is specific antibodies. Conventional methods mostly target single protein detection in formalin-fixed paraffin-embedded tissues, while mIHC/mIF technology can simultaneously target multiple proteins, accurately detecting 2-50 markers at the single-cell level, covering multiple technical platforms, such as standard IF microscopy supporting 4-5plex detection, multispectral technology for 6-8plex detection, and high-plex detection technologies such as MIBI-TOF, IMC, and DSP. These technologies have their own advantages and disadvantages and all require optimization and validation. This literature proposes consensus recommendations for best practice requirements to ensure data quality.
II. Research Content and Methods
SITC formed a multi-disciplinary expert working group, through reviewing research results, integrating experimental experience, combining multi-platform technical validation, systematically analyzing key links of mIHC and mIF technologies and summarizing and comparing technical parameters, finally forming consensus optimal operation specification recommendations. The core research content includes: comparing the advantages and disadvantages of traditional detection methods with mIHC and mIF technologies, clarifying the latter's advantages in multi-marker detection, spatial distribution analysis, and prediction of anti-PD-L1 treatment response. Clarifying key points for antibody selection, putting forward specific recommendations for monoclonal antibody priority selection, antibody validation, sensitivity and reproducibility. Standardizing requirements for experimental optimization and control settings, clarifying control setting standards and optimization directions for each experimental link. Detailed analysis of the principles, advantages, disadvantages and applicable scenarios of 5 types of mainstream mIHC and mIF technologies, clarifying the core validation requirements for mIHC and mIF detection in clinical and scientific research to ensure research reproducibility and transparency.
III. Core Research Results
1. Multiplex Chromogenic Immunohistochemistry Staining
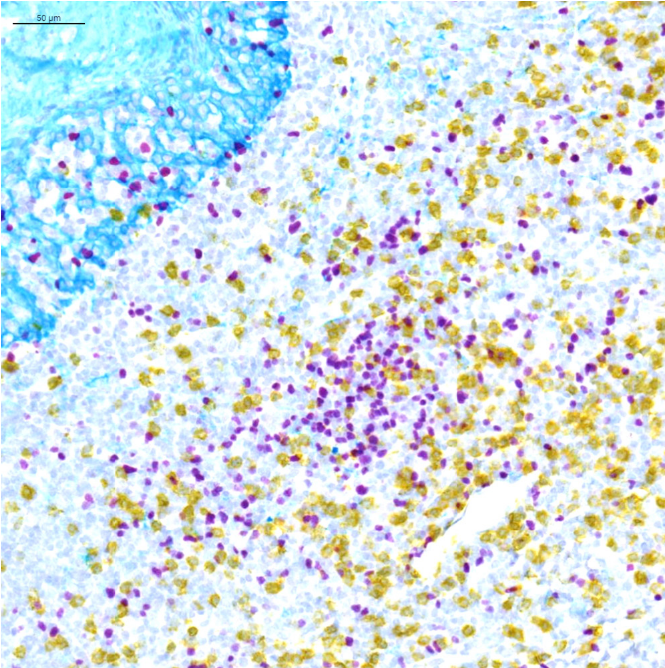
Standard chromogenic mIHC is an extension of traditional single IHC technology, achieving simultaneous detection of multiple markers on the same section through different color chromogens, suitable for routine clinical detection. This figure shows the imaging effect of triple chromogenic mIHC, validating its feasibility for multi-marker co-expression detection and chromogen distinguishability and staining clarity. Using three different color chromogens from Ventana company, supplemented with hematoxylin counterstain to distinguish cell nuclei and cell morphology, different colors correspond to the expression positions of three markers, allowing observation of marker spatial distribution differences and co-expression signals through color overlay, intuitively reflecting its multi-marker detection capability. This image validates the practicality of multiplex chromogenic mIHC, demonstrates the effectiveness of the selected chromogen combination, provides compatibility with optical microscope interpretation methods familiar to clinical pathologists, and provides a directly applicable reference for subsequent optimization of multi-marker chromogenic mIHC in clinical practice.
2. Multiple Immunohistochemical Consecutive Staining on Single Section (MICSSS)
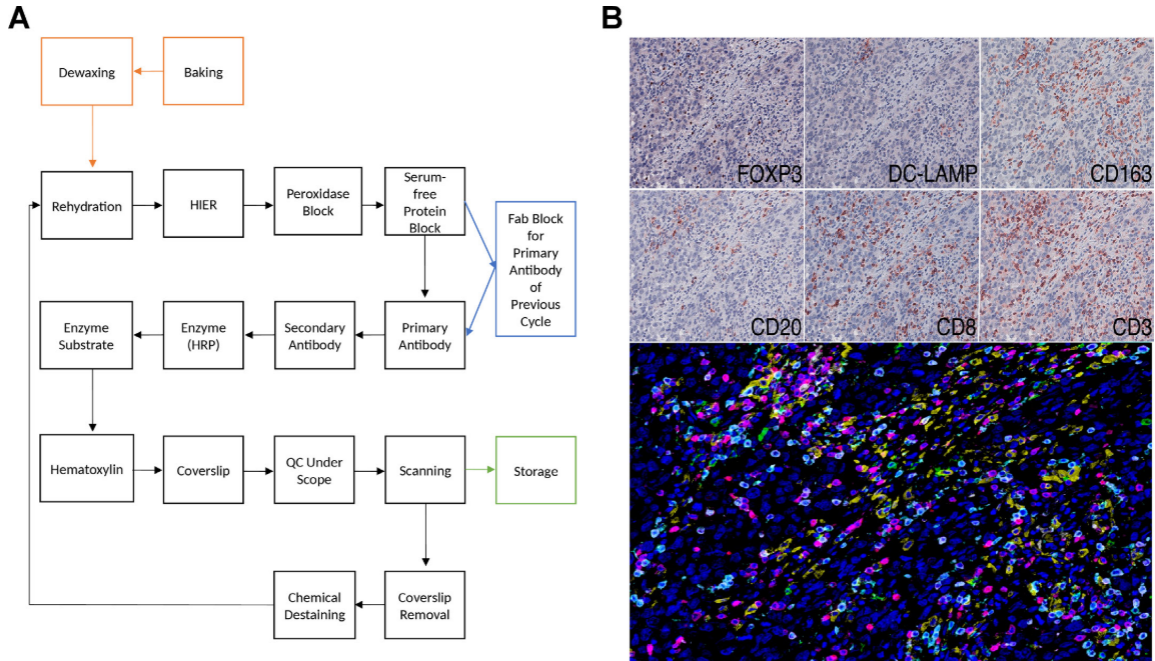
The core of MICSSS technology is to complete the detection of multiple markers on the same tissue section through "staining - scanning - destaining" cycle steps. It has strong compatibility with traditional IHC technology and can achieve simultaneous detection of multiple markers, but has the disadvantages of cumbersome operation process and longer time consumption. The figure clearly shows the complete experimental steps of MICSSS, while presenting its imaging effect in detecting multiple markers in triple-negative breast cancer tissue. Subfigure A details the cycle process from staining to destaining, including key steps such as Fab fragment blocking and chemical destaining. Subfigure B shows both the individual staining images of 6 markers and the composite pseudocolor image after fusion of these images. Individual staining images have clear signals without messy background, while composite images allow intuitive observation of the infiltration of different immune cells in tumor tissue and the spatial positional relationships between these cells. The MICSSS experimental process provides reproducible operation reference for subsequent researchers, and also proves that this technology can effectively detect multiple markers and is compatible with traditional single IHC technology.
3. Imaging Area Differences in Multiplex Staining
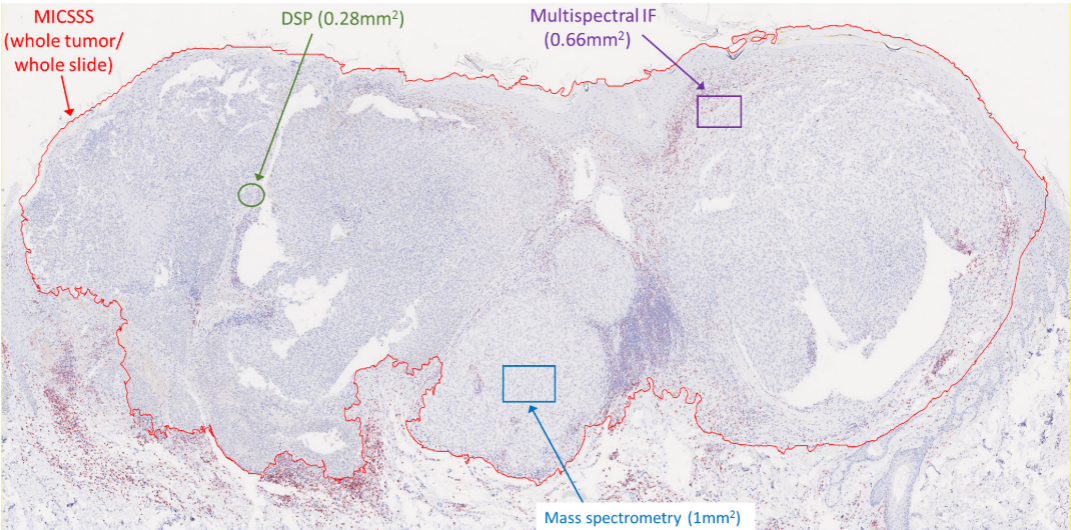
The imaging area differences of different mIHC/mIF technologies directly affect their application scenarios. Whole-section imaging is suitable for routine clinical screening, while ROI imaging is suitable for in-depth analysis of complex tumor microenvironments in scientific research. This figure uses malignant melanoma tissue as the research object, aiming to intuitively compare the imaging area sizes of 5 types of mainstream technologies to provide reference for researchers' technology selection. This figure is a representative image of malignant melanoma tissue sections, overlaid with imaging area annotations of various technologies, where MICSSS is whole tumor/whole section imaging, and multispectral mIF, EMS-IHC, and DSP are ROI imaging of 0.66mm², 1mm², and 0.28mm² respectively. The figure notes that the three ROI imaging technologies can achieve whole-section imaging through ROI stitching, but this is not widely applied currently. This image intuitively distinguishes the imaging characteristics of various technologies, reveals the differences in their application scenarios, explains the applicable scenario differences between MICSSS and mass spectrometry analysis, DSP, and also suggests the technical optimization direction of ROI stitching to achieve whole-section imaging.
4. TSA Multiplex Immunofluorescence Technology
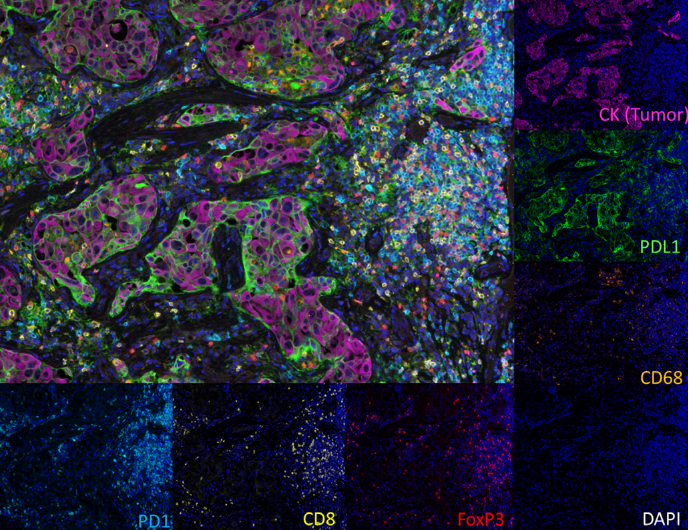
mIF combined with TSA technology can achieve signal amplification and improve detection sensitivity for low-expression markers. Multispectral microscopy can correct autofluorescence and signal overlap, enabling precise phenotypic analysis at the single-cell level. The experiment used non-small cell lung cancer tissue as the detection object, adopting TSA signal amplification and multispectral imaging to simultaneously detect 6 markers, using multi-channel imaging mode to avoid fluorescence overlap, and can display marker images individually or in combination, clearly presenting the cellular localization and co-expression of each marker. It not only validates the technical advantages of TSA-based multispectral mIF, demonstrates its detection precision, but also provides a basis for predicting anti-PD-L1 treatment response, while providing a directly referable experimental protocol for similar mIF detection in other tumor types.
5. Tissue-Based Mass Spectrometry Analysis
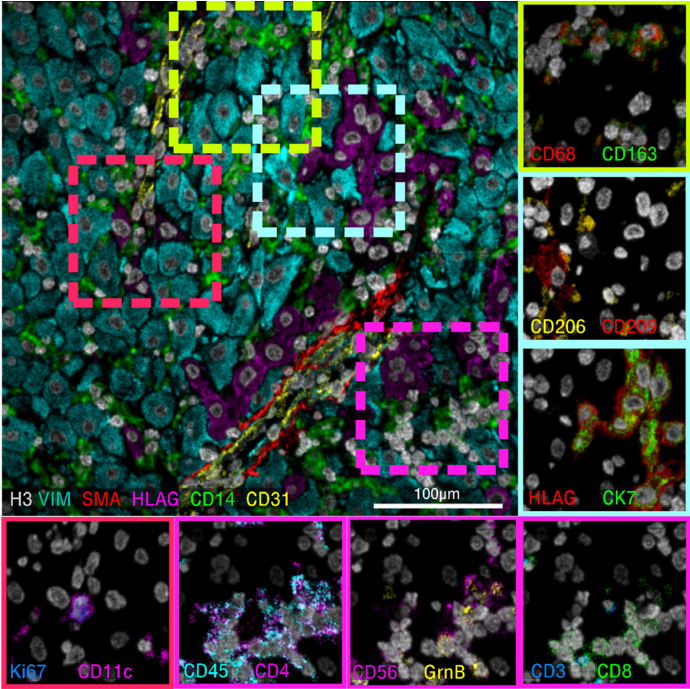
EMS-IHC uses primary antibodies combined with elemental mass tags, utilizing mass spectrometers to achieve pixel-level ionization analysis, which can simultaneously detect dozens of markers with less interference, suitable for high-dimensional analysis of complex tumor microenvironments. This figure shows its imaging effect, validating its ability for simultaneous detection of multiple markers in human decidual tissue and high-resolution spatial distribution analysis. The experiment used MIBI-TOF technology to detect human decidual tissue, applying a 40-marker detection panel, and showing imaging results of 6 markers, including a 6-color overlay main image and two-color magnification insets. The main image shows the overall spatial distribution of markers, while the insets present colocalization relationships. Grayscale image pixel intensity corresponds to marker expression abundance, enabling precise quantification with high imaging resolution. This image highlights the high-resolution spatial analysis capability of EMS-IHC, providing a tool for analyzing cellular heterogeneity in complex tissue microenvironments, while expanding the application scenarios of this technology, which can be used for exploring immune-related disease mechanisms in non-tumor tissues.
6. Digital Spatial Analysis
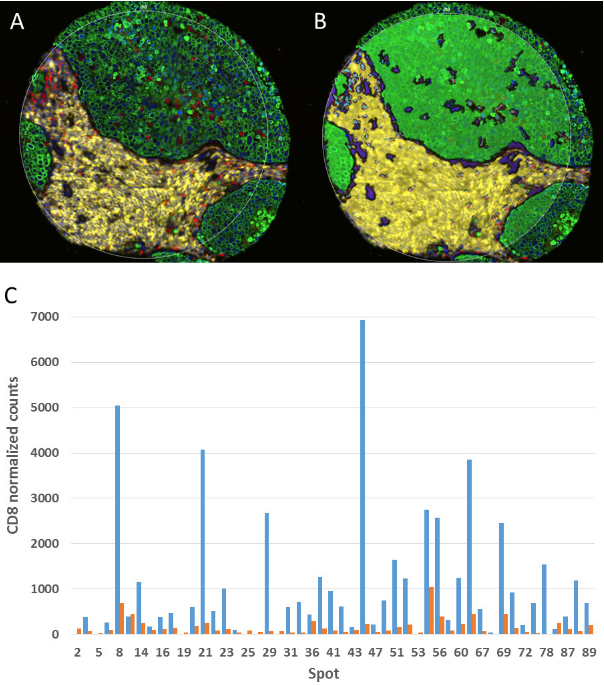
DSP technology combines UV-cleavable fluorescent DNA-tagged primary antibodies with NanoString technology to achieve precise quantification of multiple markers in specific tissue regions, without iterative staining and no autofluorescence interference, suitable for specific region analysis of clinical samples. The experiment validated its feasibility and accuracy in quantitative analysis of markers in specific regions of non-small cell lung cancer TMA. This figure clearly presents the key process of fluorescent labeling to define tissue regions, UV laser cutting of tags, and NanoString counting. The CD8 marker regional quantification results are consistent with known biological characteristics, validating quantitative accuracy. The core advantage of DSP technology lies in solving the limitation that traditional technologies cannot achieve precise localization and quantification, validating its quantitative reliability, while demonstrating its application potential in TMA high-throughput detection, suitable for multi-center clinical research and precision immunotherapy biomarker screening.
IV. Summary and Outlook
For the current 5 types of mainstream mIHC/mIF technology platforms, this literature provides detailed analysis of the principles, processes, advantages and limitations of each platform, and systematically compares them through tables. In terms of technical optimization and validation specifications, the literature proposes clear core principles, based on single chromogenic IHC detection as the basis and reference, mIHC/mIF detection needs to reproduce the results of single IHC. At the same time, it clarifies key optimization links, including antigen retrieval conditions, antibody incubation time and concentration, blocking steps, signal amplification methods, etc., which need to be optimized through matrix systems to improve signal-to-noise ratio. The validation process needs to cover accuracy, precision, and reproducibility, and when technical processes, antibody combinations or labeling methods change, re-validation is required.
mIHC/mIF technology has become a standard tool for biomarker research and is expected to enter routine clinical applications in the near future. Different technology platforms have their own advantages and disadvantages, complementing each other. Single staining technology is easier to apply to clinical practice quickly, while multiplex staining technology is still mainly used for research exploration. In the future, it is necessary to promote the standardization and normalization of technology through unified best practice specifications, while solving existing limitations through technological innovation, further exerting the core value of mIHC/mIF technology in cancer immunotherapy biomarker screening, treatment response prediction, prognosis assessment, and mechanism exploration.
References
Taube JM, Akturk G, Angelo M, Engle EL, Gnjatic S, Greenbaum S, Greenwald NF, Hedvat CV, Hollmann TJ, Juco J, Parra ER, Rebelatto MC, Rimm DL, Rodriguez-Canales J, Schalper KA, Stack EC, Ferreira CS, Korski K, Lako A, Rodig SJ, Schenck E, Steele KE, Surace MJ, Tetzlaff MT, von Loga K, Wistuba II, Bifulco CB; Society for Immunotherapy of Cancer (SITC) Pathology Task Force.. The Society for Immunotherapy of Cancer statement on best practices for multiplex immunohistochemistry (IHC) and immunofluorescence (IF) staining and validation. J Immunother Cancer. 2020 May;8(1):e000155. doi: 10.1136/jitc-2019-000155. Erratum in: J Immunother Cancer. 2020 Jun;8(1):e000155corr1. doi: 10.1136/jitc-2019-000155corr1. PMID: 32414858; PMCID: PMC7239569.
EnkiLife mIHC TSA Kits
Product | Catalog Number |
|---|---|
TSA Six-Label Seven-Color Multiplex Immunohistochemistry Kit | |
TSA Five-Label Six-Color Multiplex Immunohistochemistry Kit | |
TSA Four-Label Five-Color Multiplex Immunohistochemistry Kit | |
TSA Three-Label Four-Color Multiplex Immunohistochemistry Kit | |
TSA Two-Label Three-Color Multiplex Immunohistochemistry Kit |